Categories:
Spine Surgery Technology
Tags:
SI joint fusion Spine surgery
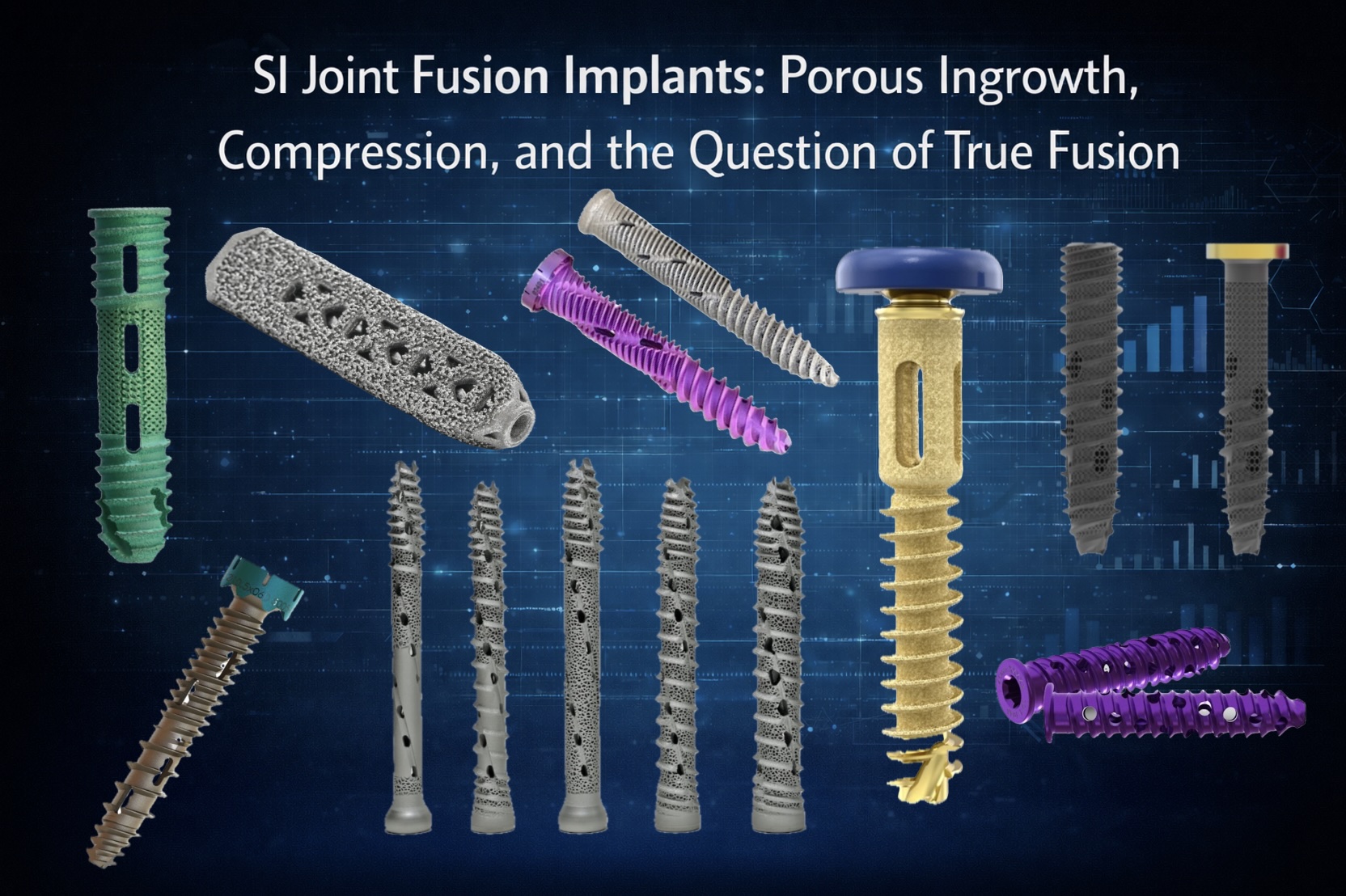
Lateral percutaneous SI joint fusion has evolved quickly — but the implants themselves may be asking a question we haven’t fully answered.
Are we solving a mechanical problem, or a biologic one?
Newer lateral SI implants increasingly emphasize 3D-printed porous architecture, designed to promote bony ingrowth and long-term integration. Others prioritize compression across the SI joint, aiming for immediate stability with the assumption that fusion will follow.
Both approaches make sense — but they reflect different philosophies.
The same tension exists in how we think about grafting:
• Fenestrated screws that allow limited graft passage
• Versus implants that create a true graft channel spanning the joint
In some cases, stabilization alone appears sufficient for symptom relief. In others, the lack of robust bone continuity across the SI joint raises questions about durability and long-term outcomes.
Which raises a broader, uncomfortable question:
If fusion is truly the goal, are we grafting enough bone across the SI joint?
And should we be more seriously considering posterior dowel grafting — either as an adjunct in select patients, or as part of a staged fusion strategy — rather than relying solely on lateral fixation and fenestration?
There’s no consensus answer here.
But implant design may be subtly steering practice patterns more than data.
I’m interested in how others are thinking about this:
– Do you prioritize porous ingrowth or compression?
– Do you believe fenestration is sufficient for fusion?
– Have you incorporated posterior grafting in select cases — or avoided it entirely?
As with many spine technologies, the most useful insights may come from shared experience rather than specifications.